Our Products
MERES100 BIORESORBABLE SCAFFOLDS (BRS)
Overview of BRS
Currently used metallic drug eluting stents stays permanently in blood vessels This may not only lead to increased risk of adverse events year on year, but may also pose a hindrance if future procedures need to be performed in the same artery. However, newer type of stents, called bioresorbable scaffolds (BRS) provides a temporary scaffold to the lesion to restore the blood flow, once the vessel blockage is treated and healing is completed, BRS dissolves fully, leaving the artery in its natural state with no foreign residue. This provides both physicians and patients the room to explore future treatment interventions, if required, in the same blood vessel..
Evolution of PCI
Invention of plain ‘old’ balloon angioplasty (POBA) indicated the first revolution in the treatment of CAD through the skin. Despite successful dilation and coronary flow restoration to the diseased coronary artery, interest in this innovative technology was lost by issues related to acute vessel closure caused by vascular elastic recoil occurred in 5–10% of patients immediately after the procedure, and development of neointimal proliferation with restenosis occurred in ~30% of patients within the first six months.
Bare metal stents (BMS) began the second revolution in the treatment of CAD as a resource to overcome the restrictions of POBA. Though, BMS resolved the issue of acute vessel occlusion, it was accompanied by major problem of in-stent restenosis (ISR). Though studies have proven that BMS implantations were superior to balloon angioplasty alone but in-stent restenosis due to neointimal proliferation was still high at the rate of 20–30%
Drug eluting stents (DES) – the third revolution in PCI – were considered as tools to solve the treatment-related issues of BMS and reduce the restenosis risk. Landmark evidence of the first generation sirolimus-eluting stents established significant reduction in vessel wall thickening due to the healing response and risk of restenosis versus the BMS. Later, the indications for DES rapidly arose, with the use of DES accepted in more complex CAD and higher risk patient groups. Despite the favorable results associated with the first generation DES, safety issues also arose, especially the risk of late stent thrombosis. The crucial concerns with the first generation DES were related 1) to the absence of biocompatibility of the drug eluting polymer causing a long-standing inflammation beyond the drug eluting period of the device, 2) to a risk of a continued scar tissue formation and risk of a ‘late-catch up’ phenomenon and late ISR, and 3) to a delayed/incomplete healing, and risk of late/very late stent thrombosis. Additionally, other issues were identified including abnormal vessel movement, explained by the endothelial layer’s abnormal function.
Even newer generation DES, did not fully resolve these concerns, especially the longer term risk of DES failure due to long-term inflammation in the vessel wall caused by the stent itself, resulting in clot formation (neo-atherosclerosis).
Bioresorbable scaffolds (BRS) heralded the fourth revolution in interventional cardiology. They were ultimately designed to overcome the perceived limitations of DES by providing a temporary support to the vessel wall, whilst simultaneously allowing for the release of an anti-proliferative drug to limit the excessive response, in order to potentially allow the vessel to heal and restore its physiological function.
The promise of BRS: Unique Chemistry
The BRS is mostly composed of repeating units of bioresorbable polymers. After implantation of BRS, bonds between repeating units in the polymer structure of these scaffolds begin to get hydrolyzed producing lactic acid, which is metabolized via Krebs cycle and get converted to carbon dioxide and water.
Chemically, scaffold absorption takes place in three phases; initially water starts breaking down chemical bonds, resulting in decrease of stent’s molecular weight. In the second stage there is decline in radial strength. At third stage, residual short polymer chains diffuse out of the device to get reabsorbed into blood.
Degradation of scaffold governs mechanical performance, which is divided into three phases: during initial “Rebuilt phase”, it acts like a typical drug eluting stent (comparable deliverability, minimal acute recoil and high radial strength. In this phase the objective is to treat the lesion & restore blood flow.
At the Revive phase, there is breaking of connecting points, causing a decline in radial strength. this phase takes three to six months post implantation. During the last “Renew phase” the BRS becomes discontinuous and ceases to act as a scaffold. It gets completely resorbed by natural process (except the small platinum markers for future fluoroscopic identification of treated vessel) gets eliminated as as Carbon di oxide and water. Renew Phases may take 24 to 36 months.
0%
SCAFFOLD THROMBOSIS
0%
CARDIAC DEATH
0%
MYOCARDIAL INFARCTION AT 1 YEAR AND 2 YEARS
Benefits
MERES100 Angioplasty- Treatment for Coronary Artery Disease
Advantages of Bioresorbable Scaffolds (BRS)
Safety and Effectiveness of Bioresorbable Scaffolds (BRS) in Clinical Evidence
Product Specifications
| Stent material and Thickness | Bioresorbable PLLA (Poly L-lactide), 100 microns |
|---|---|
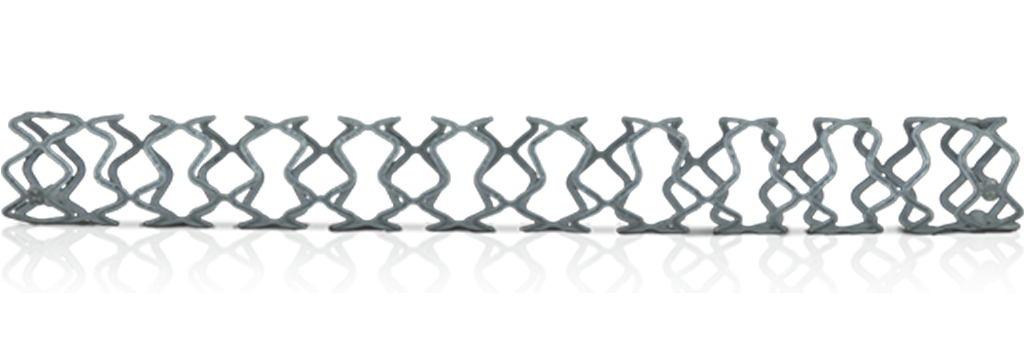
| Stent Architecture | Hybrid Design: Closed cells on ends and open cells in middle |
| Drug | Sirolimus |
| Drug Dose | 1.25μg/mm2 |
| Drug Coating | Proprietary top coat |
| Polymer | BIORESORBABLE PDLLA (POLY D, L-LACTIDE) |
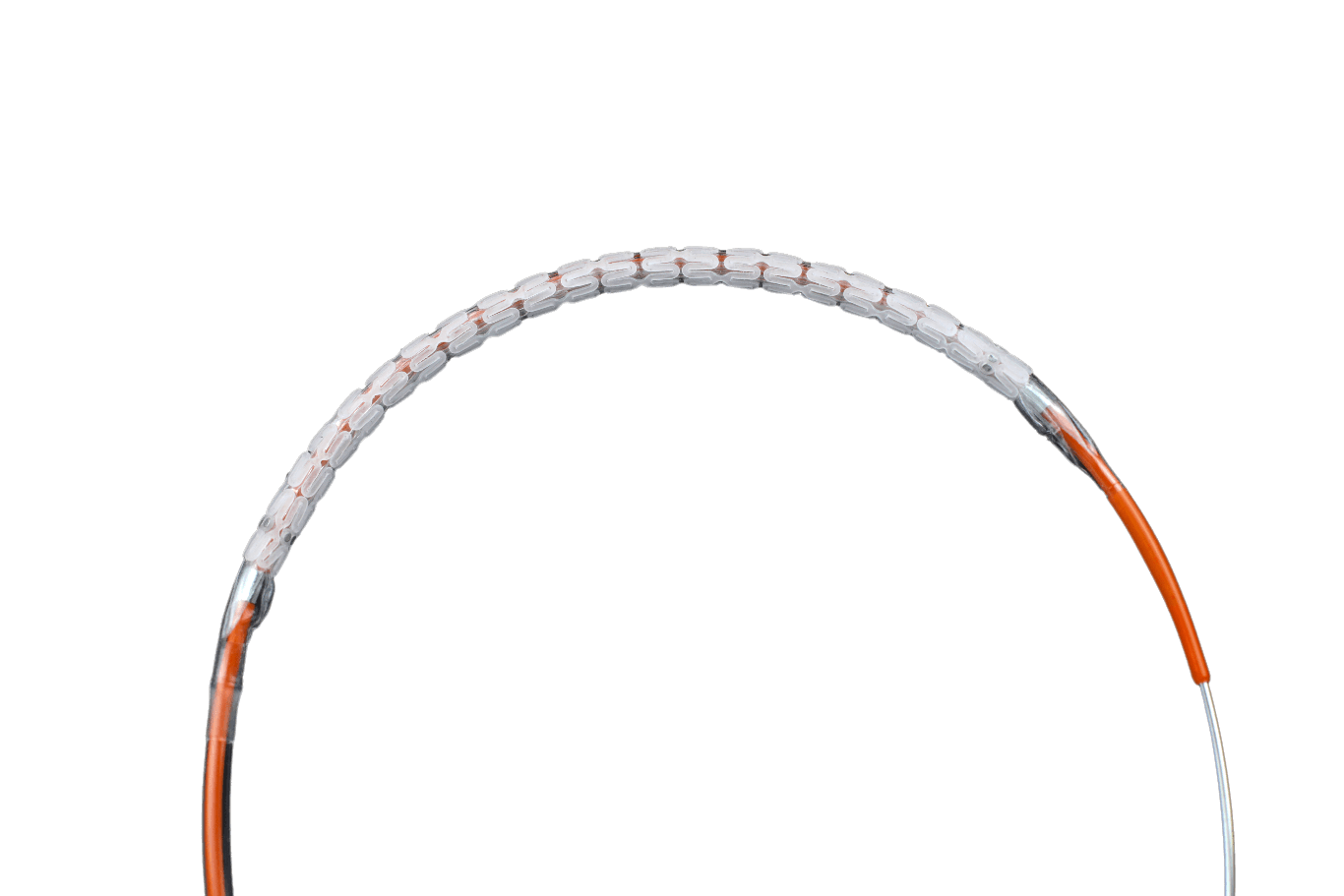
| Delivery system | Rapid Exchange |
Size Chart
| DIAMETER / LENGTH | 13 MM | 16 MM | 19 MM | 24 MM | 29 MM | 32 MM | 37 MM | 40 MM | |
|---|---|---|---|---|---|---|---|---|---|
| 2.50 mm | MRS25013 | MRS25016 | MRS25019 | MRS25024 | MRS25029 | MRS25032 | MRS25037 | MRS25040 | |
| 2.75 mm | MRS27513 | MRS27516 | MRS27519 | MRS27524 | MRS27529 | MRS27532 | MRS27537 | MRS27540 | |
| 3.00 mm | MRS30013 | MRS30016 | MRS30019 | MRS30024 | MRS30029 | MRS30032 | MRS30037 | MRS30040 | |
| 3.25 mm | MRS32513 | MRS32516 | MRS32519 | MRS32524 | MRS32529 | MRS32532 | MRS32537 | MRS32540 | |
| 3.50 mm | MRS35013 | MRS35016 | MRS35019 | MRS35024 | MRS35029 | MRS35032 | MRS35037 | MRS35040 | |
| 4.00 mm | MRS40013 | MRS40016 | MRS40019 | MRS40024 | MRS40029 | MRS40032 | MRS40037 | MRS40040 | |
| 4.50 mm | MRS45013 | MRS45016 | MRS45019 | MRS45024 | MRS45029 | MRS45032 | MRS45037 | MRS45040 | |
Clinical Data
| STUDY NAME | TYPE OF STUDY | TOTAL PATIENTS | STATUS |
|---|---|---|---|
| SPONSOR INITIATED STUDIES | |||
| MeRes-1 Study | First-in-man | 108 | Ongoing |
| MeRes-1 Extend Study | Global Study | 64 | Ongoing |